
V-V ECMO:
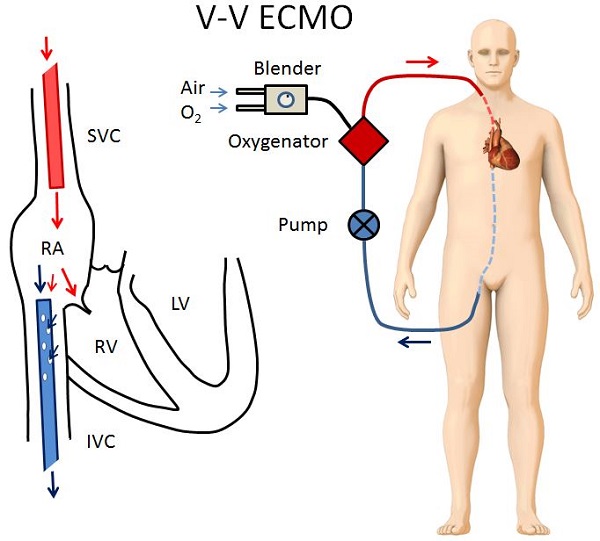
V-V ECMO is the ideal configuration for a patient in isolated respiratory failure who still has reasonable cardiac function. In V-V ECMO, the return cannula takes blood from a central vein and returns it back to the right atrium. Below are the two most common V-V ECMO configurations.
In Figure 1 the drainage cannula is inserted in the femoral vein and positioned to drain blood from the inferior vena cava as it enters the right atrium. The return cannula is inserted in the right internal jugular vein and positioned to return blood into the right atrium. In this position, a fraction of oxygenated blood from the return cannula can be sucked back into the drainage cannula before it has had a chance to circulate through the patient.
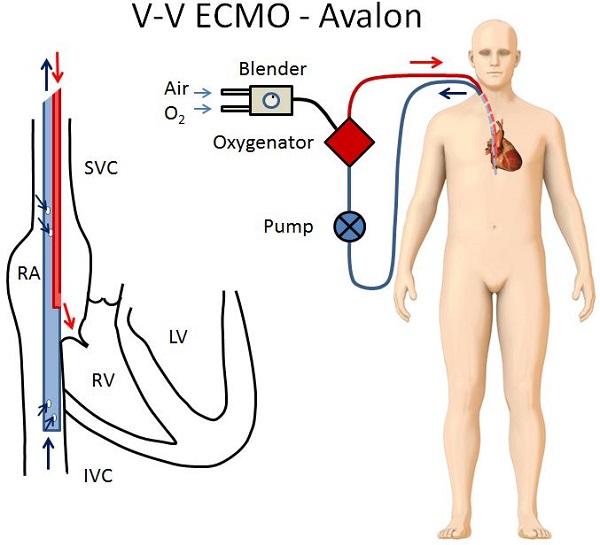
In Figure 2, a special dual lumen catheter is used, called the Avalon Catheter. It has two drainage ports and one return port. It is inserted through the right internal jugular vein, and positioned so that the two drainage ports take blood from the SVC and IVC, and the return port delivers blood into the right atrium.
Although the two configurations differ slightly, the main principles of V-V ECMO are the same:
- Deoxygenated blood is drained from a large central vein, and oxygenated blood is returned to the right atrium or another large central vein.
- The V-V ECMO circuit is connected in series with the patient’s heart and lungs, in other words it does not bypass the heart or the lungs.
- The V-V ECMO circuit provides no hemodynamic support, the patient’s native cardiac function must be intact
- The bigger the cannula, the more flow can be achieved.
- V-V ECMO is typically used in hypoxic respiratory failure. In TGH the most common reasons are:
- ARDS refractory to conventional management.
- Primary Graft Dysfunction after a lung transplant.
- Hypoxia in the context of severe lung disease as a bridge to lung transplantation.
Avalon Catheter
- The Avalon catheter is a dual-lumen cannula that only requires one site (typically the right internal jugular vein)
- The cannula is positioned so that blood is drained from the SVC and IVC and returned directly into the right atrium. (see Figure 2)
- This positioning is officially represented as (dl)V-V ECMO
- The cross sectional area is limited, so flow rates are limited to about 4 LPM.
- The main advantage is that patients can be more easily mobilized with the Avalon catheter compared to traditional V-V ECMO
- At TGH the Avalon catheter is only used in patients who are awaiting lung transplantation
- The flow rate is very sensitive to position changes
Next page: ECMO Configurations: V-A ECMO